Drug-induced lupus: which medications, which antibodies, what to do
A patient develops joint pain, pleurisy, rash, and a new positive ANA after starting a medication. Is this systemic lupus, a drug reaction, or background autoantibody noise? Drug-induced lupus matters because the answer changes management: sometimes the right treatment is not more immunosuppression, but recognizing the exposure and removing it.
Why the diagnosis is clinical, not just laboratory
Classic drug-induced lupus usually appears after months to years of exposure and improves after the culprit drug is stopped. Fever, fatigue, inflammatory joint pain, pleurisy, and a photosensitive or nonspecific rash are typical. Severe nephritis and central nervous system disease are uncommon in classic cases, which is one reason the pattern often differs from systemic lupus erythematosus. The 2019 EULAR/ACR classification criteria for systemic lupus require a positive antinuclear antibody as an entry criterion, but classification criteria are not diagnostic rules; drug timing still matters. Patients trying to understand a new antibody result may also find the overview of what a positive ANA test means helpful.
Medications most often implicated
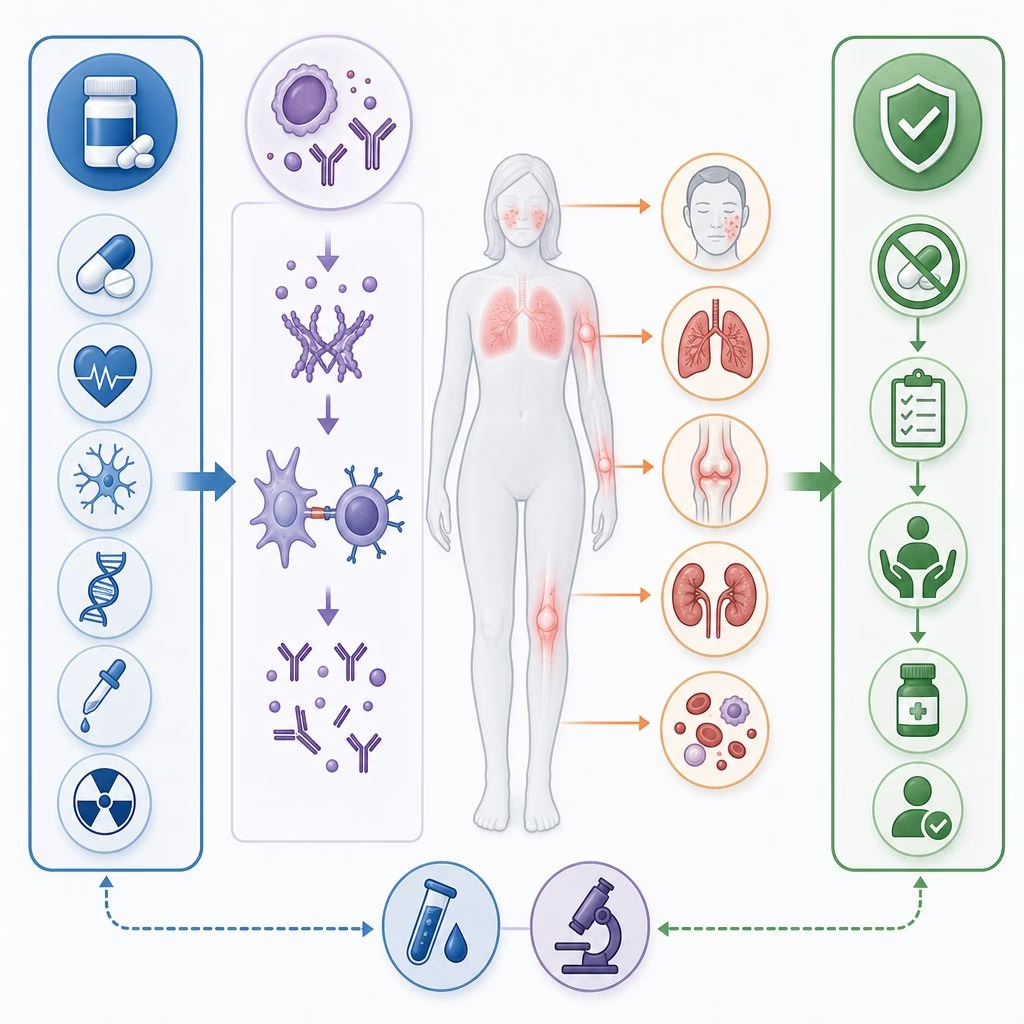
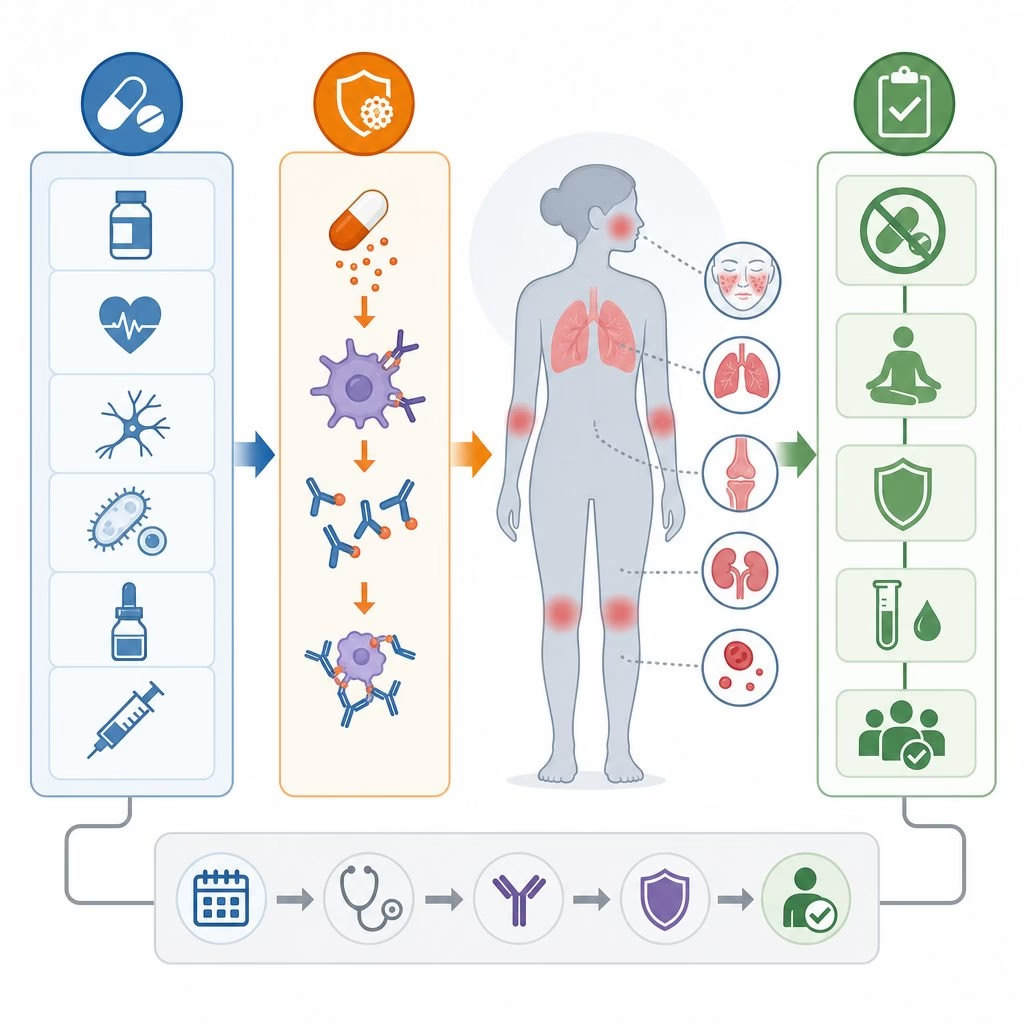
The strongest historical associations are with procainamide and hydralazine. Procainamide is now used less often, but hydralazine remains clinically relevant, especially at higher cumulative doses and in slow acetylators. Other well described triggers include isoniazid, minocycline, quinidine, chlorpromazine, methyldopa, and some antiepileptic drugs. Anti–tumor necrosis factor agents, including infliximab, adalimumab, and etanercept, can induce autoantibodies and, less commonly, a lupus-like syndrome. Interferons and immune checkpoint inhibitors can also unmask immune phenomena, though their presentations may not follow the classic pattern.
A practical example
Consider a 62-year-old taking hydralazine for resistant hypertension who develops symmetric hand stiffness, pleuritic chest pain, low-grade fevers, and a new positive ANA after two years of therapy. Normal urinalysis and complements, plus positive anti-histone antibodies, make drug-induced lupus plausible. If the same patient had heavy proteinuria, low complement levels, and anti-dsDNA antibodies, the concern for idiopathic lupus nephritis or hydralazine-associated vasculitis would rise.
Which antibodies help, and where they mislead
Antinuclear antibody is positive in most cases, often with a homogeneous pattern, but ANA positivity alone is not disease. Anti-histone antibodies are common in classic drug-induced lupus, reported in many series in more than 75% of cases, yet they also occur in idiopathic lupus. Anti-dsDNA antibodies are less typical in classic hydralazine or procainamide disease, but are more frequent with anti-TNF–associated lupus. Complement consumption, meaning low C3 or C4 from immune complex activity, is usually absent in classic cases and should prompt a broader evaluation; the related discussion of complement levels in lupus and vasculitis explains why that distinction matters.
Serologic patterns to know
What to do when drug-induced lupus is suspected
The first step is disciplined medication chronology: start dates, dose changes, cumulative exposure, and symptom onset. Testing should match the clinical question. Reasonable evaluation often includes ANA by immunofluorescence when available, anti-histone, anti-dsDNA, extractable nuclear antigen antibodies, C3 and C4, complete blood count, creatinine, liver enzymes, urinalysis, and urine protein assessment. Chest imaging or echocardiography may be appropriate when pleuritis or pericarditis is suspected.
When the presentation is mild and the suspected medication has a safe alternative, stopping the drug is the central intervention. Symptoms often improve over weeks, while antibodies may persist for months. Nonsteroidal anti-inflammatory drugs or short courses of glucocorticoids are sometimes used for arthritis or serositis, individualized to comorbidities. Hydroxychloroquine may be considered when symptoms are persistent or the diagnosis overlaps with idiopathic lupus, but it is not a substitute for removing a likely trigger.
Misconceptions that cause harm
One misconception is that drug-induced lupus is always benign. Most cases resolve, but hydralazine can also be associated with antineutrophil cytoplasmic antibody vasculitis, kidney injury, and pulmonary hemorrhage; that is a different risk category. Patients with vasculitic features may need a different evaluation, including the type of reasoning discussed in ANCA vasculitis treatment decisions. Another misconception is that every biologic-induced autoantibody requires stopping effective therapy. In anti-TNF treatment, ANA or anti-dsDNA seroconversion is common enough that, without compatible symptoms, routine antibody surveillance can create noise rather than clarity.
Frequently Asked Questions
How is drug-induced lupus different from systemic lupus?
Drug-induced lupus is usually linked to a medication exposure and often improves after the culprit drug is stopped. Classic cases are less likely to cause severe kidney or central nervous system disease than systemic lupus, but the pattern must be reviewed carefully.
Which antibody is most associated with drug-induced lupus?
Anti-histone antibodies are commonly associated with classic drug-induced lupus, but they are not perfectly specific. ANA, anti-dsDNA, complements, urine testing, and the clinical timeline all matter.
What is the first step when drug-induced lupus is suspected?
The first step is to review medication timing and whether the suspected medication can be safely stopped or replaced. Treatment decisions should also screen for kidney, lung, blood, and serosal involvement.
Where the evidence leaves us now
Evidence supports a pragmatic approach: recognize compatible symptoms, identify a credible exposure, document supportive antibodies, screen for kidney, lung, blood, and serosal involvement, and stop the likely culprit when feasible. Uncertainty remains around genetic susceptibility, dose thresholds for newer agents, and distinguishing anti-TNF lupus from evolving idiopathic disease. The harder question is which abnormal tests represent disease, not merely immune surveillance alone.