IL-6 Inhibition in RA: Mechanism, Monitoring, and Differentiating the Agents
Choosing an interleukin-6 (IL-6) inhibitor for rheumatoid arthritis is rarely about memorizing another biologic name. It is about recognizing a cytokine pathway that drives synovitis, fatigue, anemia of inflammation, thrombocytosis, and C-reactive protein (CRP), then monitoring intelligently when that same pathway is pharmacologically silenced. For patients, the practical question is: why would my rheumatologist choose this medication after methotrexate or another biologic? For referring clinicians, the question is how to interpret labs, infection signals, and disease activity when IL-6 blockade changes the usual inflammatory readouts.
Why IL-6 matters in rheumatoid arthritis
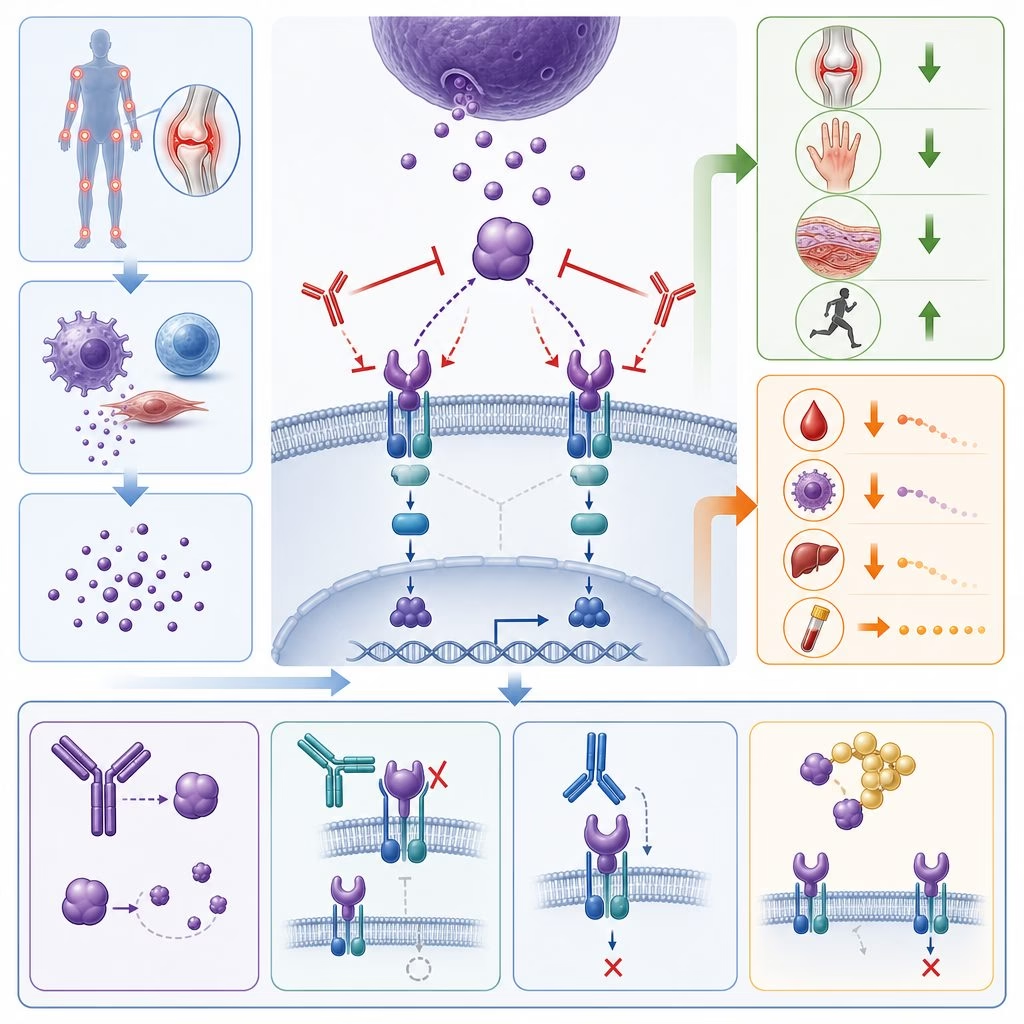
IL-6 is not the only driver of RA, but it is unusually broad in its effects. It promotes B-cell maturation, T-cell differentiation, osteoclast activation, hepatic acute-phase reactants, and the constitutional symptoms many patients describe as “the flu without a fever.” Blocking the IL-6 receptor can therefore improve joint counts and global symptoms while rapidly lowering CRP and erythrocyte sedimentation rate (ESR).
The evidence base is mature. Tocilizumab showed efficacy in methotrexate-inadequate responders in OPTION and in biologic-experienced patients in RADIATE. Sarilumab improved signs and symptoms in MOBILITY and TARGET. Head-to-head trials are also informative: ADACTA showed tocilizumab monotherapy outperforming adalimumab monotherapy, and MONARCH showed sarilumab monotherapy outperforming adalimumab monotherapy. These data matter because IL-6 inhibition is one of the few biologic strategies with credible monotherapy performance when methotrexate is not tolerated.
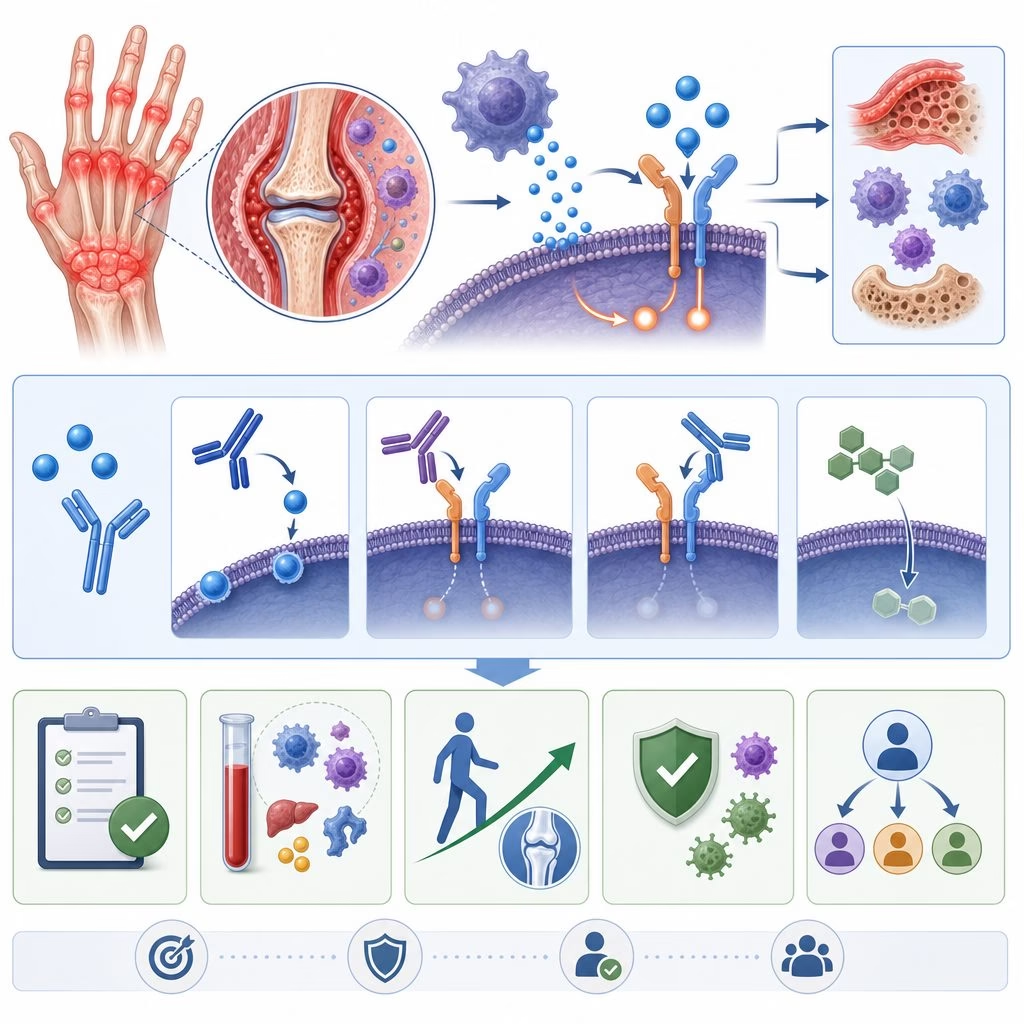
Mechanism: receptor blockade, not general immune shutdown
Tocilizumab and sarilumab bind the IL-6 receptor, inhibiting both classic signaling through membrane-bound receptors and trans-signaling through soluble receptors. That distinction helps explain their systemic effect. They do not erase the immune system; they interrupt a specific communication channel that amplifies inflammation. The result can be substantial improvement in Clinical Disease Activity Index (CDAI), a composite score that does not require CRP, which becomes important during follow-up.
Monitoring: what changes, and what can mislead
Before treatment, clinicians generally screen for tuberculosis and hepatitis, update appropriate vaccines, review infection history, and document baseline complete blood count, liver enzymes, and lipids. During therapy, the FDA labels and common rheumatology practice emphasize periodic monitoring of neutrophils, platelets, alanine aminotransferase and aspartate aminotransferase, and lipid panels.
Key monitoring principles
- CRP and ESR may normalize quickly, even when residual synovitis persists.
- Fever and CRP responses to infection can be blunted, so history and examination carry more weight.
- Mild lipid increases are expected; cardiovascular risk should be managed conventionally, not reflexively used to abandon therapy.
- Neutropenia often reflects margination rather than marrow failure, but thresholds still matter for dosing and safety.
Differentiating the available agents
In the United States, the practical comparison is usually tocilizumab versus sarilumab. Both are biologic disease-modifying antirheumatic drugs that target the IL-6 receptor, and neither should be combined with another biologic DMARD or a Janus kinase inhibitor because immunosuppression becomes additive.
Small differences in formulation, dosing intervals, insurance requirements, injection comfort, and infusion access often decide the real-world choice more than theoretical efficacy. Prior diverticulitis, chronic liver enzyme elevation, recurrent infections, uncontrolled hyperlipidemia, or baseline cytopenias may push selection toward another RA class.
A clinical scenario
Consider a 58-year-old patient with seropositive RA, persistent wrist and metacarpophalangeal swelling, morning stiffness, and a CDAI in the high-moderate range despite methotrexate. Anti-CCP positivity and erosive disease suggest a low tolerance for ongoing inflammation. If nausea limits methotrexate escalation, an IL-6 inhibitor is reasonable to discuss because the monotherapy data are stronger than for many alternatives.
Three months later, CRP is undetectable, but two swollen joints remain and the patient still struggles opening jars. That is not treatment failure by laboratory definition, nor is it remission. It is a signal to examine the joints, calculate CDAI, check safety labs, review adherence, and decide whether time, dose adjustment, or switching mechanism best fits the pattern.
Where the evidence stands
Current ACR and EULAR treatment recommendations support biologic DMARDs, including IL-6 inhibitors, after inadequate response to conventional synthetic DMARDs, with shared decision-making around comorbidities and preferences. The uncertainty is not whether IL-6 blockade works; it does. The open questions are sequencing, biomarker prediction, and how best to interpret muted inflammatory markers without missing infection or undertreating active synovitis safely in practice today.