Tapering Biologics in RA: What the Evidence Supports
For many people with rheumatoid arthritis (RA), the best appointment is the one where the disease is quiet and the next question is practical: can we safely use less medicine? Tapering biologic disease-modifying antirheumatic drugs (bDMARDs) matters because long-term therapy is expensive, inconvenient, and associated with infection risk. For clinicians, it also raises a risk calculation: undertreatment can mean pain, steroid exposure, disability, and structural joint damage.
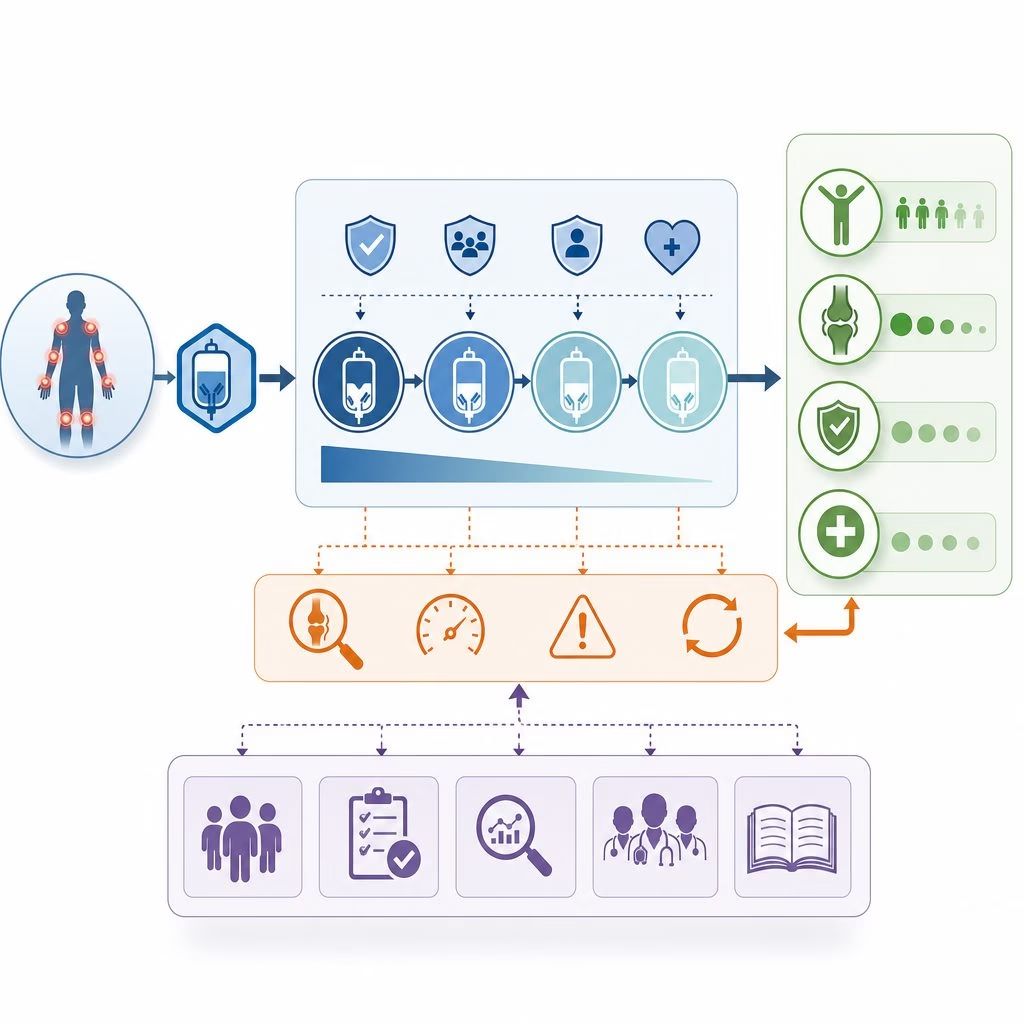
The evidence supports tapering only in selected patients who have sustained remission or very low disease activity. It should not be a reflex after one good visit, and it should rarely mean abrupt stopping. The clinical task is deciding whether inflammation has been suppressed deeply enough to reduce treatment without giving synovitis room to return.

Evidence starts with treat-to-target
Modern RA care is built on treat-to-target: measure disease activity, adjust therapy, and aim for remission or low disease activity. The 2021 ACR rheumatoid arthritis guideline recommends that patients be at target for at least six months before any DMARD taper is considered. EULAR recommendations similarly allow dose reduction of biologic or targeted synthetic DMARDs after persistent remission, particularly once glucocorticoids have been discontinued.
Those words are practical, not ceremonial. CDAI, the Clinical Disease Activity Index, combines tender and swollen joint counts, physician global assessment, and patient global assessment. A CDAI remission score of 2.8 or less is stringent. Low disease activity is easier to reach, but less reassuring when tapering is being considered. A patient with two swollen MCP joints and an elevated CRP is not quiet simply because pain feels improved.
What randomized trials show
Several randomized studies have tested reduction strategies. In PRESERVE, patients with established RA and low disease activity on etanercept plus methotrexate often maintained control on half-dose etanercept, while withdrawal performed worse. PRIZE, conducted in early RA, showed that induction with etanercept plus methotrexate followed by reduced-dose therapy preserved remission better than stopping the biologic entirely. The RRR study of infliximab discontinuation found that some patients maintained low disease activity, but many flared, especially without deep remission.
The DRESS strategy trial used a pragmatic model: disease-activity-guided spacing of adalimumab or etanercept injections in stable RA. It reduced biologic use substantially without major average loss of disease control, but flares were more frequent and required prompt dose correction. Taken together, these studies support dose reduction or interval extension before full discontinuation.
Who is a reasonable candidate?
Tapering is most defensible when several features align. Sustained remission for six to twelve months is stronger than a single good visit. Absence of swollen joints matters more than normal labs alone. Seropositive disease, such as positive rheumatoid factor or anti-CCP antibodies, does not prohibit tapering, but it raises relapse concern, especially if erosions developed previously. Continuing methotrexate often improves the odds of success because it provides background immune control and can reduce anti-drug antibody formation with some monoclonal antibodies.
Candidate checklist
An illustrative scenario
Consider a patient with anti-CCP-positive RA previously requiring adalimumab and methotrexate. After eighteen months with CDAI remission, no swollen joints, normal CRP, and no steroid use, reducing adalimumab from every two weeks to every three weeks is evidence-consistent. The plan would include a defined reassessment window and a low threshold to return to the effective schedule if objective synovitis recurs.
Misconception: tapering means RA is cured
A common misunderstanding is that remission means RA has disappeared. Biologically, remission means inflammatory pathways are suppressed below a detectable clinical threshold; autoreactive immunity may still be present. Tapering is therefore not a test of willpower, and flare is not a moral failure. It is information about the dose required to hold the disease at target.
Another confusion is the difference between tapering and stopping. Tapering usually means lowering dose or lengthening the interval while monitoring CDAI, joint counts, function, and inflammatory markers. Stopping removes the pharmacologic brake entirely and has consistently shown higher flare rates across trials. For most patients, the evidence favors gradual reduction rather than an off switch.
Monitoring after reduction
The safest taper is reversible. Before changing a biologic, clinicians should document baseline tender and swollen joint counts, patient function, morning stiffness, and recent CRP or ESR. Follow-up within two to four months is typical because many relapses declare themselves early. Imaging is not mandatory for everyone, but musculoskeletal ultrasound can help when symptoms and examination disagree.
Why partial reduction often makes more sense
Biologic DMARDs suppress specific inflammatory pathways, such as TNF signaling, IL-6 receptor activity, T-cell costimulation, or B-cell depletion. The goal of tapering is not to prove that the pathway is irrelevant; it is to find the least intensive regimen that still keeps synovitis controlled. Interval extension is attractive because it preserves the same drug and mechanism while lowering exposure. It is also easy to reverse if the examination worsens.
What the evidence supports now
Current evidence supports tapering biologics in RA only after sustained target achievement, usually by dose reduction or interval extension rather than abrupt discontinuation. The best candidates have deep clinical control, no swollen joints, no recent steroid need, and a clear rescue plan. Uncertainty remains about biomarkers that predict success, drug-specific tapering schedules, and how targeted synthetic DMARDs, including JAK inhibitors, should be reduced. The principle is durable: measurable disease control should guide decisions first, and tapering should be treated as a monitored adjustment, not a declaration that RA is gone. That balance is where evidence, examination, and patient goals appropriately meet in practice.