Osteoarthritis vs Inflammatory Arthritis: How Doctors Tell the Difference
When a patient says, “My joints hurt,” the most important clinical question is not simply where it hurts, but whether the pain is mechanical, inflammatory, or both. Osteoarthritis and inflammatory arthritis can overlap in age, location, and imaging appearance, yet the treatments and risks are very different. Missing inflammatory disease can allow preventable joint damage; overcalling it can expose patients to immunosuppression they do not need.
Why the distinction matters
The 2019 American College of Rheumatology and Arthritis Foundation guideline for osteoarthritis emphasizes exercise, weight management when appropriate, topical nonsteroidal anti-inflammatory drugs, and targeted injections for selected joints. By contrast, the 2021 ACR guideline for rheumatoid arthritis prioritizes disease-modifying antirheumatic drugs, usually methotrexate first, with escalation to biologic DMARDs or targeted synthetic agents when disease activity remains unacceptable. The same swollen hand may therefore lead to physical therapy and analgesic strategy, or to immune-directed therapy designed to prevent erosions.
The history is often the first test
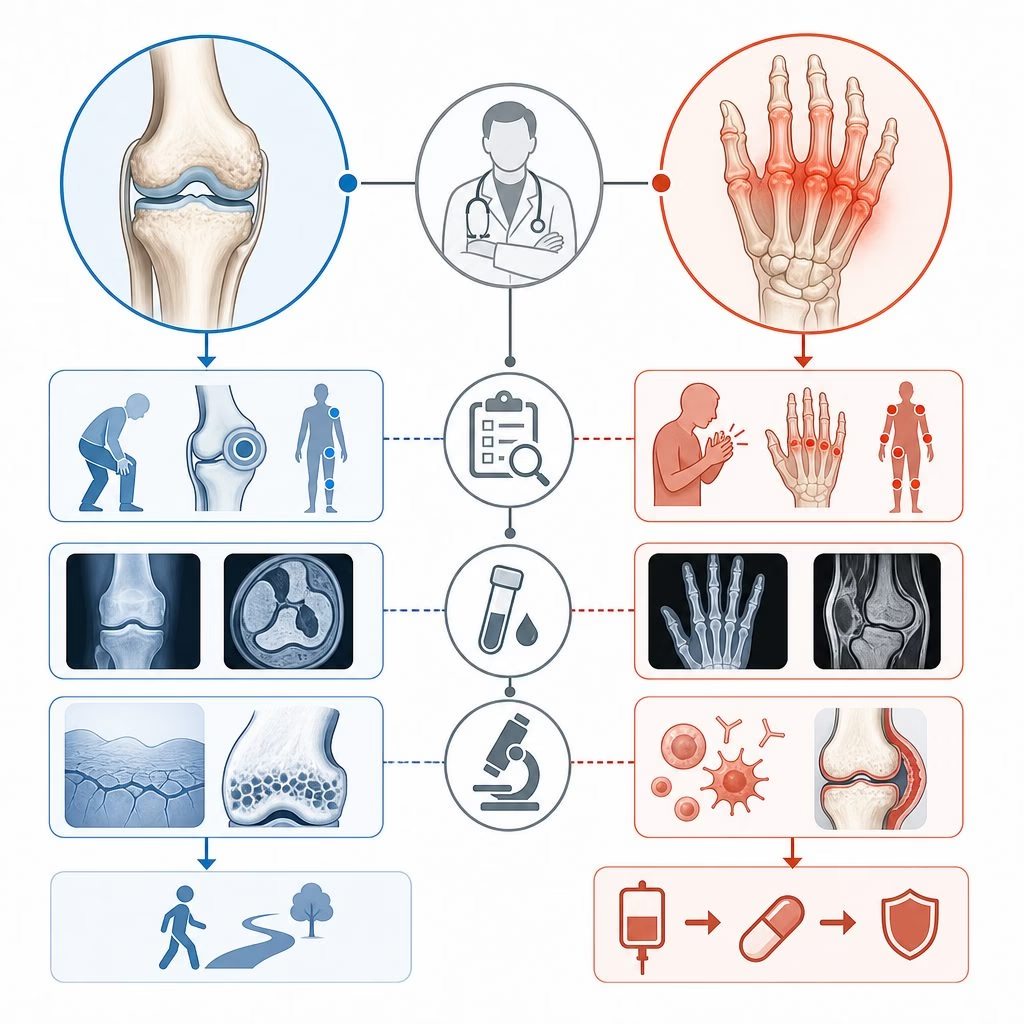
Doctors begin by listening for patterns. Osteoarthritis pain is typically use related: worse after loading, better with rest, and often concentrated in knees, hips, spine, thumb bases, or distal finger joints. Morning stiffness can occur, but it usually loosens within 30 minutes. Inflammatory arthritis tends to announce itself differently: prolonged morning stiffness, improvement with movement, night pain, and visible swelling in small joints, wrists, ankles, or feet.
A practical example helps. A 68-year-old runner with medial knee pain after stairs, crepitus, and no warmth most likely has osteoarthritis, even if the X-ray looks dramatic. A 42-year-old parent who wakes with two hours of hand stiffness, cannot make a fist, and has symmetric metacarpophalangeal swelling is a different problem until proven otherwise.
Examination separates pain from synovitis
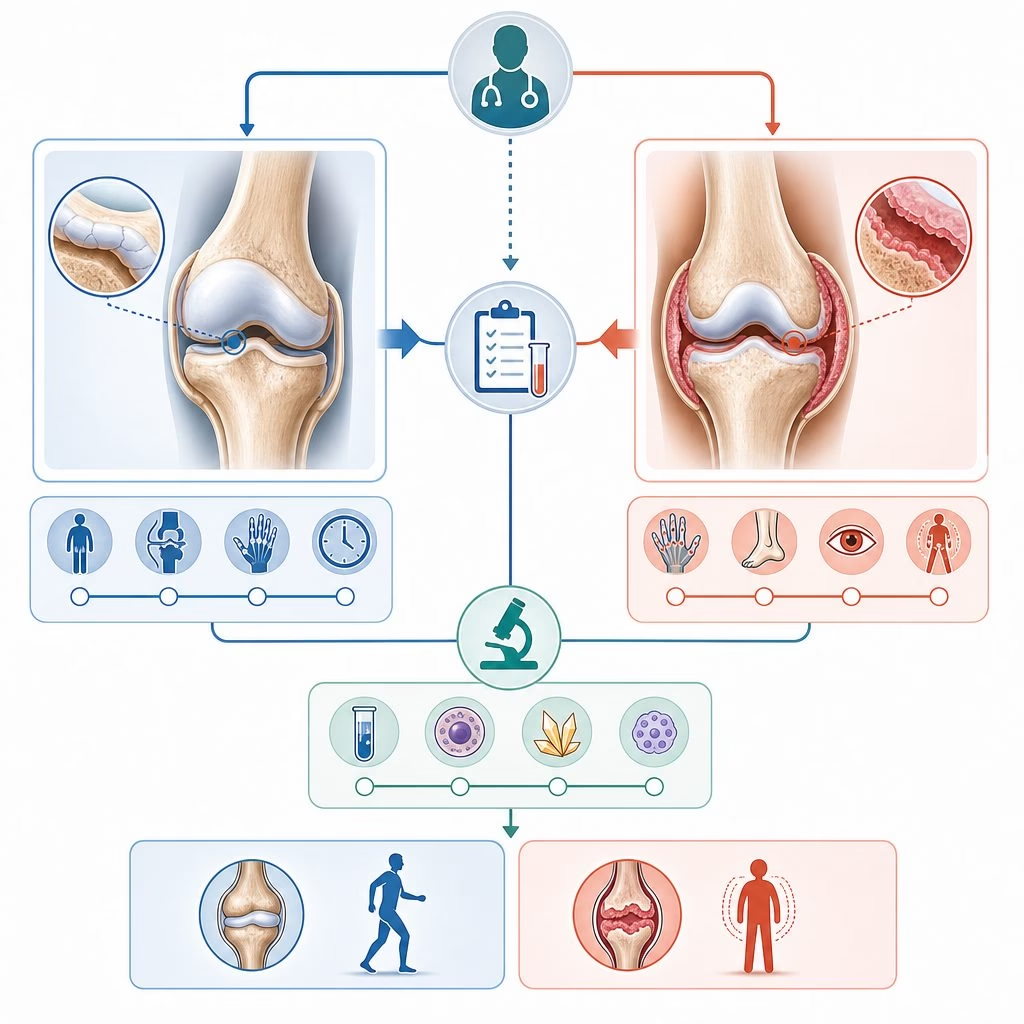
The exam asks whether the joint is tender because cartilage, bone, tendon, or biomechanics are irritated, or because synovium is inflamed. Synovitis means thickened, boggy joint lining, often with warmth and reduced range of motion from effusion. Bony enlargement, crepitus, malalignment, and pain at end range support osteoarthritis, although inflammatory flares can coexist in an osteoarthritic joint.
Pattern recognition matters
Inflammatory arthritis is not one disease. Rheumatoid arthritis commonly targets wrists, metacarpophalangeal joints, and proximal interphalangeal joints. Psoriatic arthritis may involve distal joints, dactylitis, enthesitis, or asymmetric oligoarthritis. Crystal arthritis can look intensely inflammatory but requires a different pathway. Osteoarthritis favors weight-bearing joints and mechanically stressed hand joints, but erosive hand osteoarthritis can confuse the picture.
Laboratory tests help, but they do not diagnose alone
Blood tests are useful when interpreted in context. Erythrocyte sedimentation rate and C-reactive protein measure systemic inflammation, but either can be normal in active inflammatory arthritis or elevated for unrelated reasons. Rheumatoid factor and anti-cyclic citrullinated peptide antibody, called anti-CCP, increase suspicion for rheumatoid arthritis; anti-CCP is especially specific. Antinuclear antibody testing can support evaluation for lupus or connective tissue disease, but a low-titer positive result is common and often misleading.
The ACR and European Alliance of Associations for Rheumatology 2010 classification criteria for rheumatoid arthritis combine joint involvement, serology, acute-phase reactants, and symptom duration. They were built for classification in studied populations, not as a shortcut that replaces bedside diagnosis. A patient can meet criteria and still need careful exclusion of mimics; another may fall short early and still merit close follow-up.
Imaging shows structure, inflammation, and timing
Plain radiographs remain valuable. Osteoarthritis classically produces joint-space narrowing in nonuniform compartments, osteophytes, subchondral sclerosis, and cysts. Inflammatory arthritis may show periarticular osteopenia, marginal erosions, or uniform joint-space loss, but early films can be normal. That is why a normal X-ray never rules out early rheumatoid arthritis.
Musculoskeletal ultrasound and magnetic resonance imaging can detect synovial hypertrophy, power Doppler signal, tenosynovitis, bone marrow edema, and erosions before radiographs change. Ultrasound is particularly useful at the point of care because it distinguishes fluid, synovitis, and tendon disease dynamically. Imaging should answer a clinical question; scanning every painful joint without a hypothesis creates noise.
The misconception: arthritis means wear and tear
One common misunderstanding is that age decides the diagnosis. Older adults can develop new rheumatoid arthritis, polymyalgia rheumatica, vasculitis-associated arthritis, or crystalline synovitis. Younger adults can have osteoarthritis after injury, hypermobility, congenital hip disease, or heavy occupational loading. Another misconception is that osteoarthritis is never inflammatory. Local cytokines, macrophages, and synovial activation contribute to osteoarthritis pain; however, it is not the same systemic autoimmune process targeted by DMARDs.
That distinction explains treatment logic. Osteoarthritis care tries to reduce load, improve muscle control, relieve pain, and preserve mobility. Inflammatory arthritis care tries to suppress pathologic immune activity early enough to prevent irreversible structural damage and extra-articular complications. Treat-to-target strategies use measures such as the Clinical Disease Activity Index, or CDAI, to adjust therapy toward remission or low disease activity.
When diagnoses overlap
Many referrals are not binary. A patient may have hand osteoarthritis and new rheumatoid arthritis, knee osteoarthritis plus gout, or degenerative spine disease alongside systemic lupus erythematosus. The clinical task is to identify which symptoms come from which process. Escalating immunosuppression for mechanical pain fails; dismissing persistent synovitis as degeneration also fails.
Where the evidence leaves us
Current evidence supports a disciplined approach: pattern-based history, skilled joint examination, selective laboratory testing, and imaging chosen to answer specific questions. Uncertainty remains in early disease, overlapping diagnoses, and predicting which undifferentiated arthritis will persist. The best distinction is rarely one test; it is the convergence of findings over time clinically.