Scleroderma Symptoms: Early Signs, Diagnosis, and Organ Screening
The clinical challenge in scleroderma is not only recognizing tight skin. It is deciding, early, whether vascular injury and fibrosis are quietly involving the lungs, heart, kidneys, or gastrointestinal tract. For patients, that distinction explains why a rheumatology visit may include breathing tests, an echocardiogram, antibody panels, and blood pressure review. For clinicians, it is the difference between labeling Raynaud’s phenomenon as isolated and identifying systemic sclerosis before irreversible organ damage develops.
Early symptoms that deserve a systemic lens
Systemic sclerosis, often called scleroderma, is uncommon, but missed early disease carries consequences. The 2013 ACR/EULAR classification criteria intentionally weight findings such as Raynaud’s phenomenon, fingertip ulcers or pitting scars, abnormal nailfold capillaries, sclerodactyly, telangiectasias, interstitial lung disease, pulmonary arterial hypertension, and disease-specific autoantibodies. Classification criteria are not diagnostic rules, but they reflect the clinical pattern rheumatologists use.
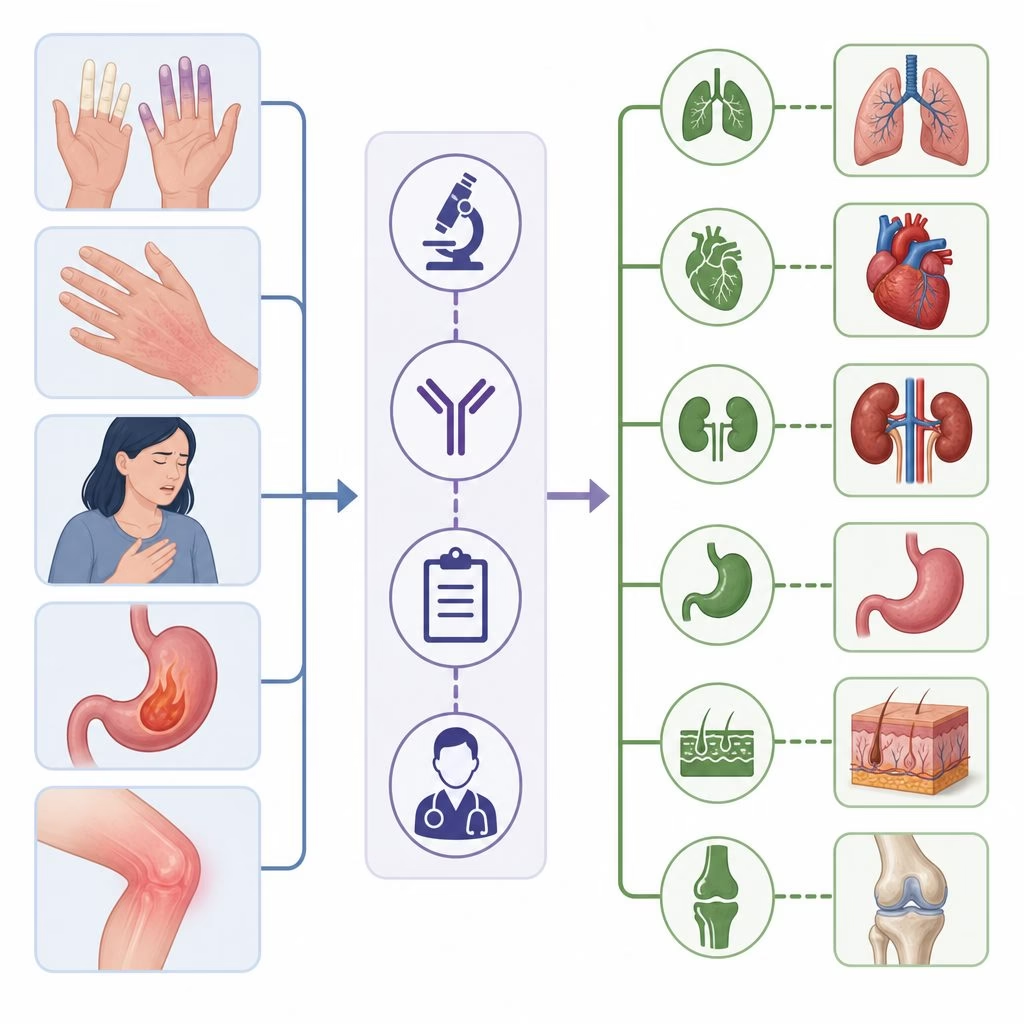
Early clues include:
- Raynaud’s attacks that are new, severe, asymmetric, or associated with ulcers.
- Puffy fingers that persist beyond morning stiffness and progress toward skin thickening.
- Reflux, trouble swallowing, early satiety, bloating, or unexplained weight loss.
- Shortness of breath, reduced exercise tolerance, dry cough, palpitations, or edema.
Why antibodies and capillaries matter
Autoantibodies help stratify risk. Anticentromere antibodies are associated with limited cutaneous disease and later pulmonary arterial hypertension. Anti-topoisomerase I, often called anti-Scl-70, is linked with diffuse skin disease and interstitial lung disease. Anti-RNA polymerase III raises concern for rapidly progressive skin thickening, scleroderma renal crisis, and temporally associated cancer in some cohorts. These associations are probabilities, not certainties, so they guide screening intensity rather than replacing clinical judgment.
Nailfold capillaroscopy is similarly useful. Enlarged capillary loops, dropout, and hemorrhages support secondary Raynaud’s and microvascular disease. A patient with winter color changes alone may need reassurance and observation; a patient with Raynaud’s, puffy fingers, anti-Scl-70 positivity, and abnormal nailfolds needs a systemic sclerosis workup.
Diagnosis is pattern recognition, not one test
A clinical example
A 42-year-old woman referred for Raynaud’s that began the prior year. She reports swollen fingers, new reflux, and breathlessness climbing stairs. Examination shows puffy hands, two fingertip pits, and fine telangiectasias. Her ANA is centromere-pattern positive, creatinine is normal, and urinalysis is bland. Even before skin tightening becomes dramatic, the pattern justifies baseline cardiopulmonary and gastrointestinal assessment.
Diagnosis usually integrates history, distribution of skin involvement, modified Rodnan skin score, nailfold findings, autoantibodies, and organ testing. The modified Rodnan skin score grades skin thickness at standardized sites; it is imperfect, but it creates a shared language for tracking diffuse disease. Clinicians should also document medication exposures, blood pressure trends, pregnancy history, occupational silica exposure, and symptoms suggesting overlap myositis or inflammatory arthritis.
Biopsy is rarely required when the phenotype is clear. Conversely, normal early skin thickness does not exclude systemic sclerosis sine scleroderma, a form with internal organ disease and minimal skin involvement.
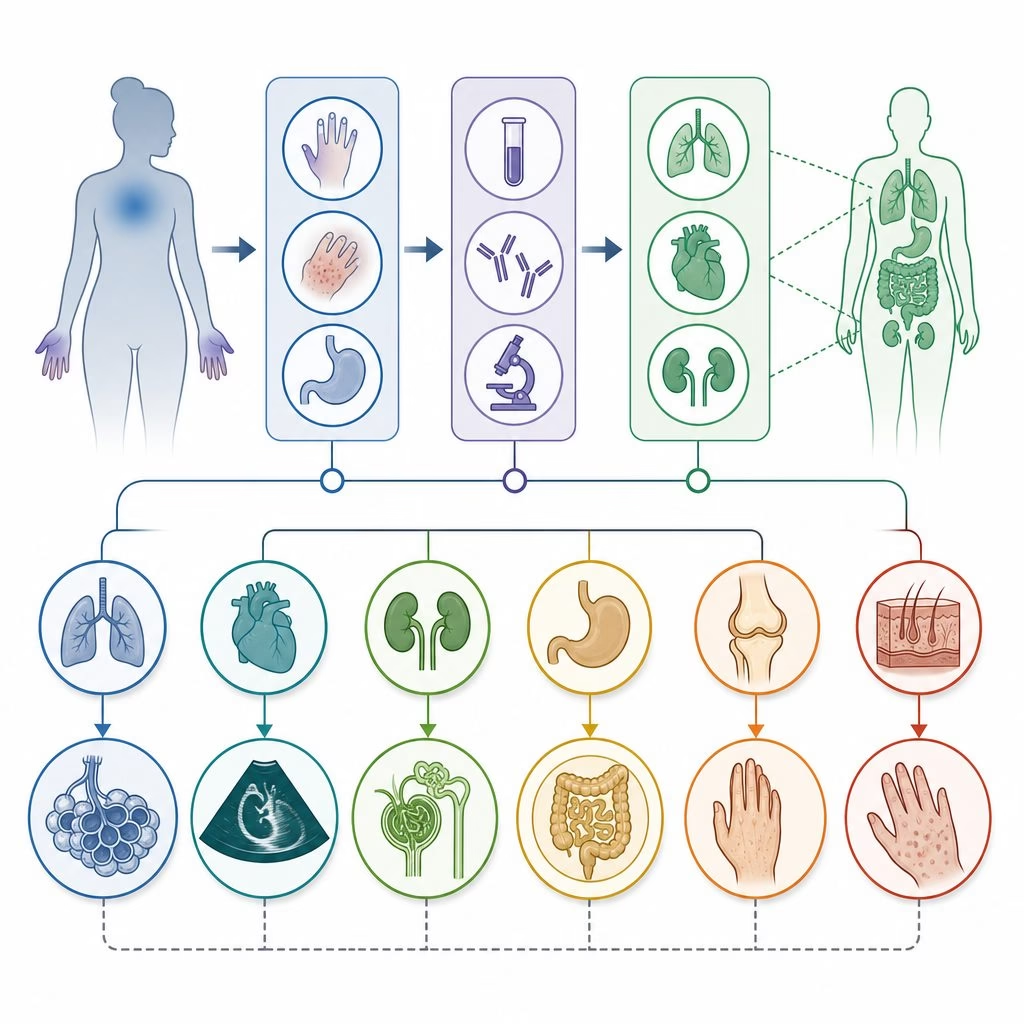
Organ screening: what rheumatologists are looking for
The 2023 EULAR treatment recommendations and contemporary pulmonary hypertension guidance emphasize proactive surveillance because symptoms may lag behind damage. Screening is not defensive medicine; it is how clinicians find treatable disease while physiology is still modifiable.
Pulmonary function tests are especially important. A falling forced vital capacity or diffusing capacity for carbon monoxide, known as DLCO, may signal interstitial lung disease or pulmonary vascular disease. High-resolution CT is more sensitive than chest X-ray for early fibrosis. For progressive systemic sclerosis-associated interstitial lung disease, randomized trials support mycophenolate mofetil as a standard immunosuppressive option, and the SENSCIS trial showed that nintedanib slows annual forced vital capacity decline. The point is not to treat every abnormality aggressively; it is to identify progression accurately.
Renal crisis, steroids, and a key misconception
One misconception is that scleroderma is primarily a skin disease, so organ testing can wait until symptoms appear. Renal crisis proves otherwise. It can present with abrupt hypertension, acute kidney injury, microangiopathic hemolytic anemia, headache, or visual symptoms. Risk is higher in early diffuse disease, anti-RNA polymerase III positivity, rapidly progressive skin thickening, and exposure to moderate or high-dose glucocorticoids.
Angiotensin-converting enzyme inhibitors transformed renal crisis outcomes once crisis occurs, but using them prophylactically in normotensive patients has not shown the same logic and may obscure rising blood pressure. The practical lesson is disciplined monitoring: home blood pressure review, renal labs, and careful steroid stewardship.
Treatment decisions start with phenotype
There is no single scleroderma medication because the disease is heterogeneous. Skin, lung, vascular, gastrointestinal, and renal manifestations respond to different strategies. Methotrexate may help inflammatory skin disease in selected patients. Mycophenolate is often favored when skin disease and lung risk intersect. Vasodilators, endothelin receptor antagonists, phosphodiesterase-5 inhibitors, prostacyclin pathway therapies, and anticoagulation decisions belong to specific vascular contexts, especially pulmonary arterial hypertension or digital ischemia. Autologous stem cell transplantation has evidence in carefully selected severe diffuse disease, but selection is critical because treatment-related risk is real.
Synthesis
Evidence supports early pattern recognition, structured organ screening, phenotype-matched treatment, and research into prediction.